Choosing the right heart valve is one of the most important decisions a patient can make. Mechanical vs tissue valves, Coumadin, durability, TAVR, and why “less invasive” is not always the best long-term solution. Every patient deserves an honest conversation about lifetime strategy, not just the next procedure.
Transcript
Today I want to explain one of the most important and often confusing decisions patients face when they need a heart valve replacement: what kind of heart valve should I choose? Let me break it down for you.
In general, there are two major categories of prosthetic heart valves. The first is what we often refer to as a mechanical valve. Technically, there is nothing mechanical about them. They simply open and close as the heart beats and relaxes. They are not made of metal either. They are made of a pyrolytic carbon compound.
These carbon valves are extremely durable and can often last a lifetime. That is terrific. In fact, I often kid my patients that these carbon compounds are so durable that when the Martians return millions of years from now, or maybe next year, they will be able to carbon date them by their carbon prosthetic heart valves.
The trade-off with these carbon valves, or mechanical valves, is that patients need to take blood thinners, specifically warfarin, also known as Coumadin. I talk about this in another video. Patients have to take these blood thinners for the rest of their lives because mechanical valves can form blood clots in the bloodstream. That means regular blood testing and careful management.
The second category of valves is known as bioprosthetic valves, often called tissue valves. These are usually made from cow or pig valves, though we sometimes use human cadaver valves.
The advantage is that most patients do not need blood thinners. You do not need to be on warfarin unless you are taking it for another reason, such as AFib. The trade-off, however, is durability. Tissue valves wear out over time, especially in younger patients, so they do not necessarily last forever.
To summarize, the two major types of valves are mechanical and biologic.
Mechanical valves typically last a lifetime but require lifelong anticoagulation. Biological valves generally do not require anticoagulation, unless needed for another condition, but they do not last forever, particularly in younger people. In some younger patients, they may last only 8 to 10 years before another procedure is needed.
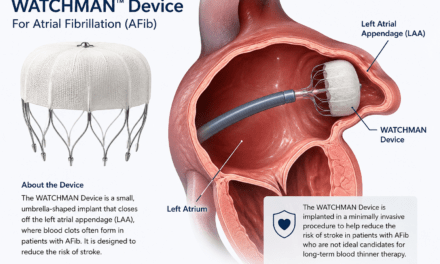
That brings us to the TAVR valve that you have heard so much about, the transcatheter aortic valve. TAVR valves are also biological valves, but instead of being sewn in during open-heart surgery, they are delivered percutaneously by catheter, usually through the groin.
TAVR has been a tremendous advance, especially for older patients or those who are too high risk for surgery. However, we have to be careful about long-term planning because recent studies have highlighted an important concern.
TAVR is now being used more often in younger, healthier patients, but the long-term durability of these valves remains a major issue, even more so than with conventional biological valves.
Many patients choose TAVR because it sounds easier. It is certainly less invasive. But if that valve is placed in a young patient and fails only a few years later, the next operation can become much more complex than if they had chosen traditional surgery in the first place. You can see how this may become a problem.
That does not mean TAVR is bad. It means the decision between TAVR and conventional surgery has to be individualized.
For example, if you have an 85-year-old patient with previous open-heart surgery, TAVR is obviously an excellent option. But for a 50- or 55-year-old patient, the conversation has to be completely different because you must think not only about recovery over the next week or two, but also about the next 10, 15, or even 20 years.
The point is that the best valve is not always the newest valve or the least invasive. The best valve is the one that fits the patient’s age, anatomy, and ability to take blood thinners.
That is why patients should be evaluated by a true multidisciplinary team, including both cardiologists and cardiac surgeons, like we do here at the Bruce and Robbie Toll Heart and Vascular Institute at Jefferson Health.
You have to understand that in heart valve disease, the goal should not simply be to get the patient through the procedure. The goal is to choose the correct lifetime strategy.
Interested in my book? You can buy it on Amazon!
(𝘛𝘩𝘦 𝘷𝘪𝘦𝘸𝘴 𝘦𝘹𝘱𝘳𝘦𝘴𝘴𝘦𝘥 𝘪𝘯 𝘮𝘺 𝘱𝘰𝘴𝘵𝘴 𝘢𝘳𝘦 𝘮𝘺 𝘰𝘸𝘯 𝘢𝘯𝘥 𝘥𝘰 𝘯𝘰𝘵 𝘳𝘦𝘱𝘳𝘦𝘴𝘦𝘯𝘵 𝘵𝘩𝘦 𝘷𝘪𝘦𝘸𝘴 𝘰𝘧 𝘮𝘺 𝘦𝘮𝘱𝘭𝘰𝘺𝘦𝘳 𝘰𝘳 𝘢𝘯𝘺 𝘰𝘳𝘨𝘢𝘯𝘪𝘻𝘢𝘵𝘪𝘰𝘯.)
Recent Posts
Your Heart Was Made to Move
What is the best exercise for your heart? There isn’t just one answer. Dr. Raymond Singer explains how aerobic exercise, strength training, flexibility, balance, and simple daily movement can all support cardiovascular health.

Can Sleep Affect Your Waistline?
We often think about diet and exercise when we talk about maintaining a healthy weight. But there may be a third piece of the puzzle: sleep. Dr. Raymond Singer explores how insufficient sleep can affect hunger, metabolism, cravings, abdominal fat, and cardiovascular health.
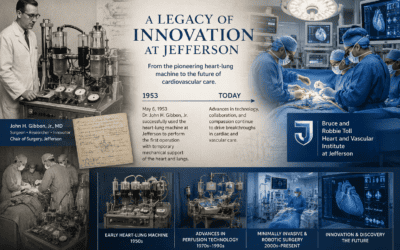
The Heart-Lung Machine: A Jefferson Legacy That Changed Medicine
More than 70 years ago, Jefferson surgeon and researcher John H. Gibbon Jr. helped make what once seemed impossible a reality: temporarily replacing the functions of the heart and lungs with a machine so surgeons could operate on a stopped heart.

50 Years Later: A Journey Home
As I prepare for my 50th high school reunion, I find myself reflecting on a journey that has taken me from Cheltenham to college, medical school, surgical training, decades of practice, and ultimately back home to care for the community where it all began.

GLP-1 Medications and Alcohol: Can They Reduce Cravings?
Emerging research suggests GLP-1 medications may do more than help with weight loss. They may also reduce alcohol cravings by influencing the brain’s reward pathways.
Heart Symptoms You Should Never Ignore
Not every symptom means heart disease, but some warning signs should never be ignored. Dr. Raymond Singer shares five important symptoms that deserve prompt medical evaluation and explains when it’s time to call 911.
Featured
Pages
- Learn about heart valves. Heart Valves
- Read testimonials. Testimonials
- Did you know I have a consulting firm? Singer Heart/Lung Consulting
- Check out my TedTalk! Defining Success
Links
- Links page with more information about your heart. Links
- Dr. Adam Pick's Site: heart-valve-surgery.com


{kind=link}