The internal anatomy of the heart is fascinating. There are four chambers of the heart. In order to go from one chamber to the next, the blood must travel across valves that keep the blood moving forward.
Here’s the path that the blood travels:
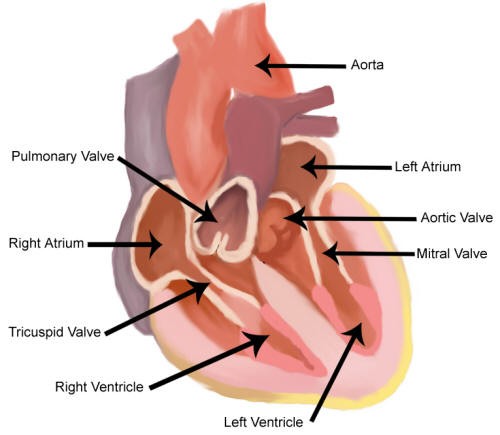
- The blood arrives into the heart through the superior and inferior vena cava and enters the right atrium.
- Then the blood passes across the tricuspid valve to enter the right ventricle.
- After leaving the right ventricle, the blood passes across the pulmonary valve and goes to the lung where the blood becomes oxygenated.
- After leaving the lungs, the blood returns to the heart and enters the left atrium.
- From the left
atrium the blood crosses the mitral valve and enters the left ventricle. - Finally, the blood leaves the left ventricle and crosses the aortic valve to enter the aortic artery and then on to the rest of the body.
Below you can click the links to learn about the four heart valves:
Aortic
Mitral
Pulmonary
Tricuspid
Click below to learn about the three different surgical approaches to valve surgery:
Conventional
Less Invasive
Trans-Catheter
External Appearance of the Heart:
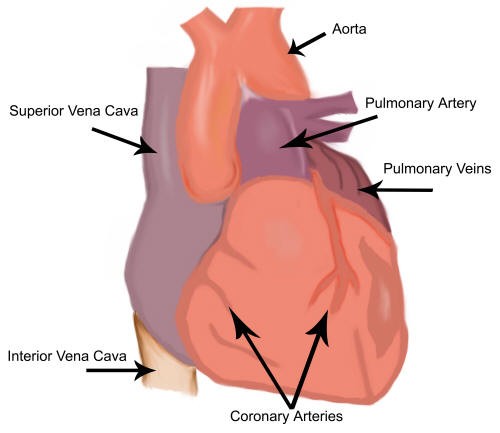
External Appearance of the Heart
Internal Structures of the Heart
Internal Structures of the Heart
Heart Valve Disease:
Below you can see my video where I discuss Heart Valve Disease:
One of the most important and often confusing decisions patients face when they need a heart valve replacement: what kind of heart valve should I choose? Let me break it down for you.
In general, there are two major categories of prosthetic heart valves. The first is what we often refer to as a mechanical valve. Technically, there is nothing mechanical about them. They simply open and close as the heart beats and relaxes. They are not made of metal either. They are made of a pyrolytic carbon compound.
These carbon valves are extremely durable and can often last a lifetime. That is terrific. In fact, I often kid my patients that these carbon compounds are so durable that when the Martians return millions of years from now, or maybe next year, they will be able to carbon date them by their carbon prosthetic heart valves.
The trade-off with these carbon valves, or mechanical valves, is that patients need to take blood thinners, specifically warfarin, also known as Coumadin. I talk about this in another video. Patients have to take these blood thinners for the rest of their lives because mechanical valves can form blood clots in the bloodstream. That means regular blood testing and careful management.
The second category of valves is known as bioprosthetic valves, often called tissue valves. These are usually made from cow or pig valves, though we sometimes use human cadaver valves.
The advantage is that most patients do not need blood thinners. You do not need to be on warfarin unless you are taking it for another reason, such as AFib. The trade-off, however, is durability. Tissue valves wear out over time, especially in younger patients, so they do not necessarily last forever.
To summarize, the two major types of valves are mechanical and biologic.
Mechanical valves typically last a lifetime but require lifelong anticoagulation. Biological valves generally do not require anticoagulation, unless needed for another condition, but they do not last forever, particularly in younger people. In some younger patients, they may last only 8 to 10 years before another procedure is needed.
That brings us to the TAVR valve that you have heard so much about, the transcatheter aortic valve. TAVR valves are also biological valves, but instead of being sewn in during open-heart surgery, they are delivered percutaneously by catheter, usually through the groin.
TAVR has been a tremendous advance, especially for older patients or those who are too high risk for surgery. However, we have to be careful about long-term planning because recent studies have highlighted an important concern.
TAVR is now being used more often in younger, healthier patients, but the long-term durability of these valves remains a major issue, even more so than with conventional biological valves.
Many patients choose TAVR because it sounds easier. It is certainly less invasive. But if that valve is placed in a young patient and fails only a few years later, the next operation can become much more complex than if they had chosen traditional surgery in the first place. You can see how this may become a problem.
That does not mean TAVR is bad. It means the decision between TAVR and conventional surgery has to be individualized.
For example, if you have an 85-year-old patient with previous open-heart surgery, TAVR is obviously an excellent option. But for a 50- or 55-year-old patient, the conversation has to be completely different because you must think not only about recovery over the next week or two, but also about the next 10, 15, or even 20 years.
The point is that the best valve is not always the newest valve or the least invasive. The best valve is the one that fits the patient’s age, anatomy, and ability to take blood thinners.
That is why patients should be evaluated by a true multidisciplinary team, including both cardiologists and cardiac surgeons, like we do here at the Bruce and Robbie Toll Heart and Vascular Institute at Jefferson Health.
You have to understand that in heart valve disease, the goal should not simply be to get the patient through the procedure. The goal is to choose the correct lifetime strategy.
Case Study – Triple Valve Replacement in a 20-Year-Old Patient
With permission from the patient and his family to post, in order to help others, this is an extraordinary case of a 20-year-old who required a triple heart valve replacement operation.
He presented with gastrointestinal symptoms, fatigue, and weight loss. His work-up showed that he had a non-ischemic cardiomyopathy with an ejection fraction at one point as low as 20%. His condition was complicated by multi-valve endocarditis, likely a variant of non-bacterial thrombotic endocarditis (NTBE), secondary to inflammation. He did not have a history of COVID or recent vaccination.
He received excellent heart failure evaluation and care by Dr. David Allen at the St. Luke’s University Hospital, in Northampton County, Pennsylvania, and he sought a second opinion with Dr. Eduardo Rame, at the Jefferson University Hospital Heart Failure Center, in Center City, Philadelphia. The patient’s ejection fraction improved to 45-50%, but he still had severe aortic, mitral, and tricuspid valve regurgitation, requiring surgery.
After seeking several surgical opinions, the patient underwent aortic valve, mitral valve, and tricuspid valve replacement surgery at the Jefferson Einstein Montgomery Hospital, in East Norriton, Pennsylvania. He also had a heart muscle biopsy performed during surgery, special cultures, and genetic testing. He recovered well, now being discharged to home on post-operative day five.
Lots of lessons, but clearly the most important is how his Mom knew something was wrong with her son after months of nonspecific symptoms and weight loss. His Mom intervened and helped her son get the answers and excellent care that he needed, including a second and third opinion. On the physician side, doctors across multiple institutions and disciplines collaborated to help this young person avoid the need for a heart transplantation. Excellent outcome for what was a scary series of events for this young patient and his family.