By far, the safest, most reliable/reproducible approach to complex valve surgery is using conventional techniques.
As I discussed in the section on coronary artery bypass surgery, the median sternotomy incision provides the best exposure to all regions of the heart and great vessels. It’s easy to perform and it’s remarkably well-tolerated.
Unfortunately, the sternal incision has been given a bad rap. People often refer to it as “cracking the chest.” Even many heart surgeons are critical of the sternal incision, particularly those who are promoting less invasive surgery. Let me take a moment to discuss two concerns about having a sternal splitting operation. The first is the concern about having pain. The second is the concern about a delay in return to normal activities.
The fact is, the sternal incision has served us well for decades and continues to be the incision of choice for most open heart procedures.

My Mom only 4 weeks after conventional aortic
valve replacement and two-vessel coronary artery bypass surgery!
By the way, my Mom was 78 years old in this picture. She never had one day of pain from her sternal incision. In fact, there were only two incisions that bothered her. The first was the puncture site for the cardiac catheterization which was black and blue for months. The second was the incision in her arm where the surgeon harvested the radial artery for one of the bypass grafts. She did complain that her hand was always cold for many year, but no pain from her sternal incision.
Rather than take my word for it, check out the videos of some of my patients below:
Let me explain why there is so little pain afterwards…
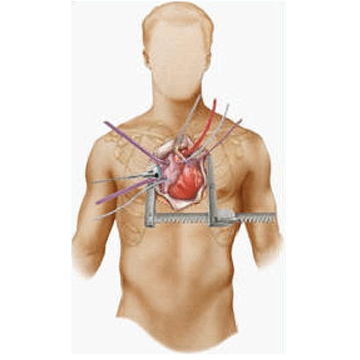
When we make a sternal incision we cut through little to no muscle. If you feel your chest in the midline, there’s nothing by skin and bone. The large pectoralis muscles are on either side of the midline. There are no major nerves in the midline either. Your nerves come from your spine and end in the midline. Ironically, most of the “less invasive” procedure utilizes an incision between the ribs. There’s a nerve under each rib (the “intercostal nerve”) which is quite painful once disturbed. Have you ever heard of the pain associated with a broken rib? It’s bad.
So, what about splitting the sternal bone? Doesn’t that hurt?
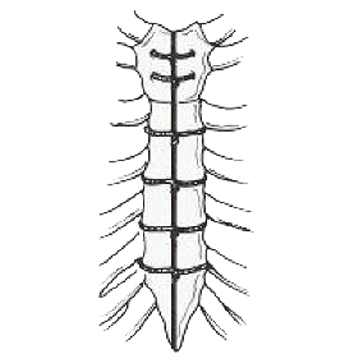
First, you have to understand that we reconstruct the bone with stainless steel wires or cables as shown below.

Stainless Steel Wires
And, like any “broken bone” once it’s “fixed” it usually doesn’t hurt too badly. I’m always impressed by how little discomfort patients have after a conventional sternotomy.
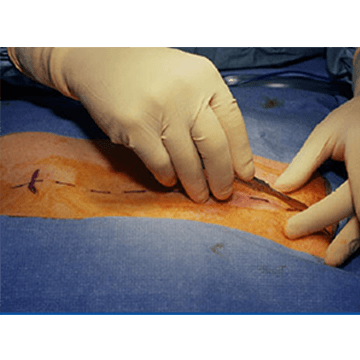
To illustrate, you can see in this photo a patient going home only four days after aortic valve replacement via the the traditional surgical approach. This approach remains an excellent choice for young patients. This is especially true for patients with congenitally abnormal valves, as in cases of aortic insufficiency (leaking valve).

As a further example, I performed mitral valve repairs in two young men, both 48 years old, on the same day using the conventional sternotomy approach. On post-operative day 1, they described their pain as “4 out of 10” mostly from the chest drains. On day 2 (with the drains removed), their pain was “2 out of 10.” They both were discharged to home on day 3 and when they returned to the office in follow-up two weeks later, both described having absolutely no pain or discomfort whatsoever.
You can see the typical look of the incision after it’s healed completely. This is about a year after his surgery. Not as brutal as some suggest.
Typical Scars
Below are pictures of the sternotomy wound in a



At home, you’ll be able to continue to walk stairs and gradually resume normal activities. We recommend not driving a car for 4 weeks and not lifting over 20 pounds for two months.
After a sternotomy, you will be awake and alert after your operation and removed from the ventilator within an hour or two later. The first evening of your surgery you’ll be sitting in a chair. By day 2 you’ll be walking in the halls and by day 3 you’ll be walking stairs and looking toward going home.
Which gets us to the final issue… When can I go back to work?
There is no doubt that after a sternotomy, you shouldn’t lift anything heaving for 2-3 months. So, if you’re in construction or if you’re required to lift heavy objects at work, you may not be able to resume full duties for 3 months. Of course, most of our patients aren’t required to do that much lifting and many of my patients return to work in 6 weeks –which is little different than my patients who have “less-invasive” techniques.
(Video above) Patient, 10 weeks after a sternotomy, doing a handstand!
Here is another example of a patient, an octogenarian, who underwent a sternotomy and felt very little pain afterwards.
Despite the positive outcomes, the debate over sternotomy versus the less invasive techniques continues. Again, I’m not someone who has stuck his head in the sand. I began performing less invasive heart procedures in 1997. A lot of patients prefer the less invasive approach and we’ve enjoyed a lot of success with less invasive techniques. It’s just not completely clear to me that it’s better than conventional techniques. Sadly, a lot of surgeons perform less invasive techniques more for marketing purposes rather than truly believing they are doing a better operation. I discussed this in my editorial on President Clinton’s heart surgery.
Nevertheless, we continue to use less invasive techniques in select patients and we’re adding new procedures every year. No doubt, there are increasing numbers of patients who are requesting less invasive approaches. And, in select cases the less invasive approach has certain advantages. I discuss this extensively on the “Less Invasive” page.