Four Types of Less Invasive Coronary Artery Bypass Surgery:
Types of Less Invasive Coronary Artery Bypass
MIDCAB:(Minimally Invasive Direct Coronary Artery Bypass Surgery)
This was the first “minimally invasive heart surgery.” And, I was the first to perform this procedure in the region on July 11, 1996. Though my experience was written about in The Morning Call and The Wall Street Journal, I responded with an editorial cautioning the public that conventional surgery was still the best choice for the overwhelming majority of patients which, indeed, turned out to be correct.
The procedure involved making a small incision, usually under the left breast. The surgeon would then sew the left internal mammary artery directly to the left anterior descending coronary artery while the heart was beating.

MIDCAB
The procedure quickly lost favor because it was limited to one bypass. It was difficult to harvest the left internal mammary artery through the small incision. And, the results were marginal at best, despite some large series showing good results. Some patients suffered complications specific to this procedure, including intercostal nerve pain, wound complications, and most of all, anastomotic complications.
Keep in mind; this once was “the hot new thing” with a report on the front page of many newspapers, but how many

MIDCAB in The New York Times
OPCAB: (Off Pump Coronary Artery Bypass)
This procedure asks the question, “What is the most invasive part of bypass surgery? Is it the incision? Or, is it the use of the heart-lung machine?” The advocates of this procedure answer by saying that the most dangerous part of bypass surgery is the heart-lung machine. Of note, I don’t agree with this philosophy but instead would say that the most important part of the operation is a perfect, complete job for which the heart-lung machine provides the best opportunity.
The technique of OPCAB uses the same incision as conventional surgery, the median sternotomy (sternal split). However, instead of stopping the heart, this procedure uses a variety of “stabilizing devices” to hold a vessel still so that the surgeon can sew to that vessel while the rest of the heart is beating. The reason these surgeons use the median sternotomy is
Here is one of the stabilizing devices that are placed on the heart:

Stabilizing Device
OPCAB has had variable acceptance. Overall, only 10-30% of all CABG procedures done in the United States are done with this technique, probably now closer to only 10%. However, there are some institutions that the surgeons have taken a particular interest in the procedure and perform 90% “off-pump.”

OPCAB
The results are also variable. Keep in mind, coronary artery bypass surgery is actually one of the most studied and of the safest surgical procedures performed with results of only 1-3% mortality and 1-5% complication rates. Imagine for a moment how difficult it would then be for any new technique to improve on these results. In fact, at best the results are as good, but not better than conventional techniques. And, personally, I do not feel the surgical anastomosis (the sewing) is as accurate because of the movement of the heart.
Below is the landmark article that showed conclusively that On-Pump (Conventional) Coronary Bypass Surgery had better outcomes than Off-Pump (Beating Heart) technique:
On-Pump (Conventional) Coronary Bypass Surgery had better outcomes than Off-Pump (Beating Heart) technique

Port-Access (Heartport®)
This technique uses the concept of making a small
The technology is extremely complex, utilizing catheters in the groin and neck. Protection of the heart is variable and there are well-documental complications unique to this technique. This technology could be used both for coronary artery bypass surgery and for valve surgery, especially mitral valve surgery.
Here are how the many catheters and tubes are placed:
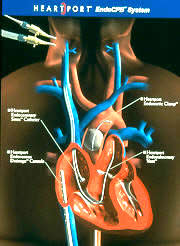
Heartport

Placement of Catheters for Heartport
This technique utilizes the use of the robot. There were originally two companies that have developed robotics for heart surgery, Computer Motion
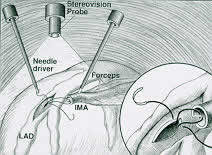
TECAB (Totally Endoscopic Coronary Artery Bypass Surgery)
Below is this first generation robot:

TECAB
In those early procedures in 1996, I harvested the left internal mammary artery using the robot and then made a small incision and performed a MIDCAB procedure. Computer Motion no longer exists. The main surgical robot is made by Intuitive Surgical and is known as the Da Vinci Robot. The newer generation robots are more complex with three to four working ports, as opposed to the one port that I used in 1996.
Robot Surgery
There are a few surgeons around the country who are using the Da Vinci robot for coronary artery bypass surgery. This requires harvesting the internal mammary artery using a thoracoscopic technique as discussed above and then performing the bypasses either with the beating heart technique or the port-access on pump technique, all through smaller incisions.
While these few surgeons are marketing the
Moreover, we already have outstanding results with conventional techniques (1% mortality, documented consistent results). It’s hard to take such a successful operation and make it much more complicated and then suggest the more complicated approach is better.
As you can see below, the newer generation robots have many more arms and instruments. The surgeon doesn’t even stand at the operating

Surgeon at the Robot
Robot Article
If they do not use the Heartport® balloon “endoclamp” (inside the aorta) to stop the heart, then they are using a conventional clamp (known as a Chitwood clamp, named after Randy Chitwood, a North Carolina surgeon who developed the clamp). This clamp is placed through yet another incision in the right chest used to directly clamp the aorta (outside the aorta) in order to stop the heart. Keep in mind; all of these incisions are made between the ribs.There has been more acceptable success using the robot for mitral valve surgery. This technique is nearly identical to the port-access (Heartport) techniques discussed above. That is to say, the surgery is done through a small incision in the right chest. In addition, an incision is made for a camera. Finally, two or three additional incisions are made for the instruments used for exposing the valve, retracting, holding sutures, etc.
Randy Chitwood is an interesting guy. He is one of the leaders involved in minimally invasive heart surgery, including robotics. However, he required coronary artery bypass surgery only a few years ago and chose to have it done by the conventional approach!
With this background, let me summarize by telling you my philosophy on these new techniques: I believe that as surgeons we need to continue to find ways to lessen the pain of surgery and enhance recovery.
In many fields, such as general surgery and gynecology, there has been great success with laparoscopic techniques which has been the standard approach now for many procedures such as gallbladder removal, appendectomy, and fertility procedures.
However, the abdomen is different than the chest. The abdomen is soft and compliant. When the general surgeon performs laparoscopy, carbon dioxide is instilled into the abdomen creating a tent with a clear view of all of the internal structures. In addition, these internal structures do not move. The gallbladder, appendix, and ovaries just sit there quietly.
The chest wall, on the other hand, is rigid, being guarded by the ribs and the sternum. The chest surgeon cannot make the chest bigger by instilling carbon dioxide. Therefore, the visualization of the organs is quite limited. In fact, the heart sits right under the sternum (breast bone) making it very difficult to work on through small lateral incisions. Special breathing tubes must be placed to collapse the lungs just to see into the chest. Most of all, everything is moving in the chest. The lungs are breathing; the heart is beating and so on. In order to stop the lungs and arrest the heart to do cardiac procedures through small incisions the techniques are often a very complicated as reflected by the problems encountered by Heartport®.
Will robotic surgery overcome these limitations in the chest? Right now, that’s the 1.8 million dollar per machine question. I would say that as always with new technology, I am cautiously optimistic; however, the reality is that the technology at this point is still in its infancy. Its advantage over conventional approaches is still yet to be proven. The fact remains that we routinely perform large numbers of complex mitral valve procedures without robots using conventional techniques with reproducible results, short hospital stays, and rapid recovery.
Even though many of the newer technologies for coronary artery bypass surgery haven’t proven to be better, it’s important that we continue to advance the science and investigate new techniques.
“Only those who dare to fail greatly can ever achieve greatly.
-Robert F. Kennedy