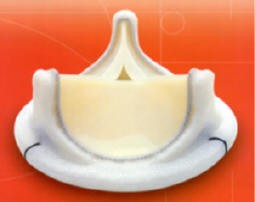
Below is a nice drawing that we made that illustrates the complexity of the internal structures of the heart.
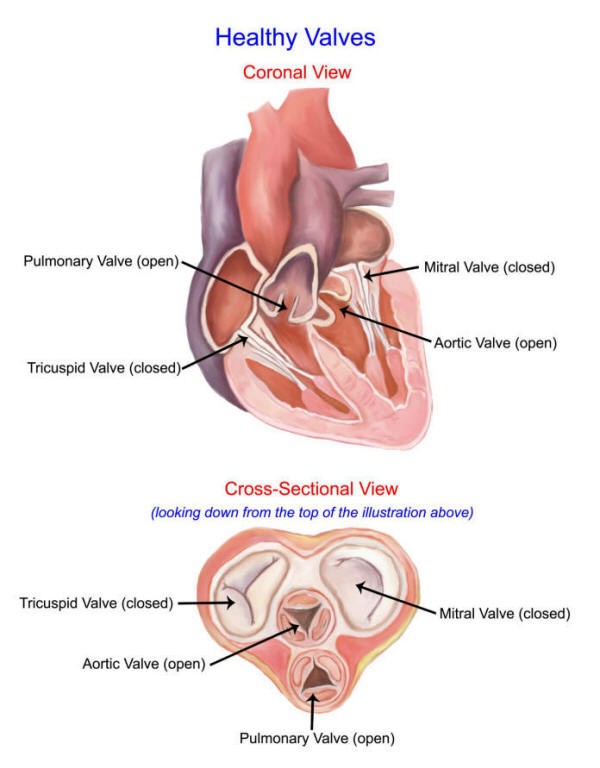
Healthy Valves
There are four heart valves.
The aortic valve sits at the base of the aorta and is the last valve the blood sees prior to being ejected from the heart. I often refer to the aortic valve as the “window of the heart” for this reason.
In order to perform complex valve surgery, the surgeon needs to be able to understand the three dimensional anatomic relationships of the heart. I believe that it was during my fellowship at Children’s Hospital in Philadelphia when I came to truly understand the anatomy of the heart and it’s variations.
While in practice, I also traveled abroad and observed some of the most famous valve surgeons in the world, like Dr. Magdi Yacoub in London and Drs. Alain Carpentier, Carlos Duran, and Christophé Acar in Paris.

Dr. Christophé Acar and Dr. Carlos Duran – Photo taken during my visit to Paris in 1999

Sir Magdi Yacoub, photo taken while I visited Dr. Yacoub in England, 1999
In adult cardiac surgery, the aortic valve is the most common valve that we perform surgery upon. There are two reasons why a valve fails. It either gets blocked (stenosis), or it leaks (insufficiency).
Aortic stenosis is the most common disease of the aortic valve, whereas mitral insufficiency (prolapse)is the most common disease of the mitral valve.
Below is an intra-operative photograph of a bicuspid aortic valve with severe stenosis secondary to calcium buildup.

Click on the above image to view it larger in another tab
Surgical Options for Valve Surgery
There are basically two options: either repair or replace the valve. Ideally, we wish we could repair all valves so that the patient is left with his/her own natural tissue. Unfortunately, we can rarely repair an aortic valve, whereas most mitral valves can be repaired.
The reason most aortic valves cannot be repaired is because the most common disease of the aortic valve is aortic stenosis which is usually caused by heavy buildup of calcium deposits as noted in the picture above. The calcium destroys the underlying valve leaving us no choice but to remove the valve with all of its calcium and replace it.
I was interviewed on Channel 69 News by the morning anchor, Eve Tannery, concerning Barbara Walters’ heart valve surgery. Barbara Walters underwent aortic valve replacement due to severe aortic stenosis.
Click on the video below!
Choices of Prosthetic (Replacement) Valves
Once again, there are two basic options: Either mechanical (metal) or biologic (tissue). So, how do you choose between the various choices of mechanical and biological valves?
Mechanical Valves
The advantages of mechanical valves
Mechanical valves (metal valves) are easy to insert generally speaking they last forever. Mechanical failures are extremely rare. They are not rejected by the body, so no special anti-rejection medications are needed.

St. Jude Mechanical Aortic Valve
The Disadvantages of mechanical valves:
Mechanical valves require the patient to take Coumadin® (a blood thinner) every day, or else the valve will develop clot that can lead to catastrophic mechanical failure and/or stroke from emboli to the brain.
Coumadin® (warfarin sodium) is a safe drug, but it has risks. Statistically, there is a 2.2% chance per year of bleeding complications and a 1.8% chance per year of clotting complications. You can have bleeding complications despite having the drug level monitored closely. Clotting can occur if the blood levels drop for some reason and it is not picked up in time.
Most of all, taking Coumadin® every day is inconvenient for the patient. You have to watch what you eat since certain foods reduce the anti-coagulation affect in your blood. Also, you will need regular blood tests, sometimes weekly, to adjust your blood levels.
Finally, mechanical valves often make a clicking sound that can be heard by the patient or by someone standing near the patient, particularly in thin people. This can be annoying to the patient and somewhat embarrassing. I tell the patients to call me if the clicking stops!
Below you can see a testimonial about why this patient opted to go for the mechanical valve.
Tissue Valves
The advantage of tissue valves:
Tissue valves do not require blood thinners, except maybe a daily baby aspirin. There is no need for Coumadin®, though some surgeons will place their patients on Coumadin® for 8 weeks after the surgery until the tissues are healed. Long-term, a daily aspirin will suffice. Therefore, the risks and inconvenience of long-term anti-coagulation is avoided.
Edwards Lifesciences Bovine Pericardial (Cow Tissue) valve
It may surprise you to know that tissue valves are not rejected by the body either and therefore do not require any anti-rejection medication, even the human valve (homograft/cadaver valve).
Also, tissue valves are silent. They don’t make any noise when they open and close.
The disadvantage of tissue valves
Tissue valves (pig, cow, or human) are slightly more challenging to insert, particularly transplanting another human valve (homograft/cadaver valve). However, an experienced surgeon should have not difficulty with any of these tissue valves. Indeed, greater than 90% of the valves I use to replace diseased valves are tissue valves.
Tissue valves do not last forever. Interestingly, the longevity of a tissue valve depends in part on the patient’s age. Young patients will develop calcium deposits more quickly on tissue valves than older patients.
For example, a pig or cow valve placed in a 35 year old patient will probably last no more than 10 years. That same valve place in a 75 year old patient will most likely last 15 or more years, which would be fine for someone that age.
As far as tissue valves go, the human valve and some of the newer chemically treated pig valves may last the longest, but this is debated in the literature.
")
Aortic Homograft (Human Cadaver Valve and a Portion of the Ascending Aorta)
My Recommendations
I look at each patient differently, though my bias is toward tissue valves. The reason I generally prefer tissue valves is because I am concerned about the long-term risks of Coumadin®.
Age is an important factor, as I alluded to above. For patients over 70 years of age, particularly if they have associated medical problems such as coronary artery disease, I will always recommend a tissue valve to replace a diseased aortic valve.
For younger patients, I try to assess the patient’s lifestyle and the patient’s concerns. I try to explain the balance between the risk of long-term anti-coagulation required with a mechanical valve versus the risk of a second operation with a tissue valve. It’s always interesting to me how each patient is different. Most of the times, the patient will make the decision on their own.
After I get done explaining all of the valve options, I let the patient think about it for a while and discuss the matter with their family. Though I give my advice, I often recite to them the line from Fox Cable News: “We report, you decide!”
Don’t get me wrong, mechanical valves are an excellent choice in select situations. For example, it is my valve of choice in a young patient with mitral valve disease that cannot be fixed by repairing the valve. There are also times when a mechanical valve is the best choice for the aortic position, too.
Fortunately, I have a large experience placing all the variety of valves available, so that I can honestly pick the right valve for the right patient. Some surgeons only feel comfortable placing certain types of valves. Ask your surgeon what the other choices are for valve replacement and inquire as to your surgeon’s experience placing all of the different valves.
Testimonial
Second Open Heart Surgery to Replace a Deteriorated Tissue Valve
With permission from the patient to post, this 68-year-old man underwent a redo-aortic valve replacement. His previous operation was an aortic valve replacement, mitral valve repair, and tricuspid valve repair. His repaired valves were still fine but the biologic prosthetic aortic valve had prematurely deteriorated, requiring him to undergo a redo-heart surgery just 4 years later.
He describes in this video how his experience of now recovering from a second heart operation was as quick, or quicker, than his first operation. In fact, many patients tell us that their second operation wasn’t as bad, in part because they knew what to expect and also because of what they have experienced in terms of the advances in heart surgery and perioperative care.
You read more about his story here.
Calcific aortic stenosis
Calcific aortic stenosis is the most prevalent heart valve disorder in developed countries. It is characterized by progressive fibro-calcific remodeling and thickening of the aortic valve leaflets that evolve over years to cause severe obstruction to cardiac outflow.
This 58-year-old patient on chronic hemodialysis for end-stage renal disease presented with acute systolic heart failure, metabolic acidosis, and hypotension. On ECHO his aortic valve area was 0.4 cm². The valve had a fixed opening and therefore the patient also had moderate-to-severe aortic insufficiency. He was stabilized and promptly taken to the operating room for surgical aortic valve replacement with a CryoLife On-X valve.
The choice of a mechanical valve was based on his young age, the fact that he was already on chronic anticoagulation, and the concern that a biological valve would deteriorate rapidly from the impact of hemodialysis.
The photograph below shows the aortic valve specimen removed intact, revealing a donut of calcium and debris, along with a small fixed opening.

Testimonials/Case Studies
With permission from the patient to post, this 64-year old woman was born with a bicuspid aortic valve. Over the years, her aortic valve became calcified and stenotic. She also had bicuspid aortopathy, resulting in an ascending aortic aneurysm.