The term “minimally invasive” has become an often misunderstood and overused phrase in cardiac surgery. Many equate it with smaller incisions or robotic approaches. But the reality is that the incision is not always what makes a heart operation “invasive” —to me, it’s operating on the heart that is the invasive part of the procedure.
When performing complex “open-heart” surgery, such as mitral valve repair, the true invasiveness arises from the fact that the heart must be stopped, opened, and supported by a heart-lung machine. Once that step is necessary, the size or location of the incision may become a secondary consideration. 𝗪𝗵𝗮𝘁 𝘁𝗿𝘂𝗹𝘆 𝗺𝗮𝘁𝘁𝗲𝗿𝘀 𝗶𝘀 𝘀𝗮𝗳𝗲𝘁𝘆, 𝗲𝘅𝗽𝗼𝘀𝘂𝗿𝗲, 𝗽𝗿𝗲𝗰𝗶𝘀𝗶𝗼𝗻, 𝗮𝗻𝗱 𝗱𝘂𝗿𝗮𝗯𝗹𝗲 𝗹𝗼𝗻𝗴-𝘁𝗲𝗿𝗺 𝗼𝘂𝘁𝗰𝗼𝗺𝗲𝘀.
Moreover, despite the derisive phrase that refers to the conventional approach as “cracking the chest,” a median sternotomy remains the gold standard for most open-heart operations. It provides consistent exposure, control, and efficiency—and can now be made smaller, with less spreading, and yes, even with minimal or no postoperative pain. I’ve demonstrated this many times in my patient videos that can be found on my website and on social media.
To be clear, I have great respect, support, and admiration for my colleagues who are advancing less invasive and robotic techniques. But my cautionary belief remains that even as the safety and experience for these technologies improve, there are valid indications for offering traditional approaches for many patients. The key is to individualize care. There is not just one procedure fits all patients.
It’s also important to understand that even less invasive procedures have risks. For example, potential risks specific to less-invasive mitral valve repair approaches may include intercostal neuralgia, diaphragm paralysis, liver injury, vascular injury, and retrograde aortic dissection. Lastly, and surprisingly, hospitalization and recovery times are not always significantly faster than traditional approaches.
In my personal experience of more than 𝟱𝟬𝟬 𝗶𝘀𝗼𝗹𝗮𝘁𝗲𝗱 𝗺𝗶𝘁𝗿𝗮𝗹 𝘃𝗮𝗹𝘃𝗲 𝗿𝗲𝗽𝗮𝗶𝗿 𝘀𝘂𝗿𝗴𝗲𝗿𝗶𝗲𝘀 𝘃𝗶𝗮 𝗮 𝘀𝘁𝗲𝗿𝗻𝗼𝘁𝗼𝗺𝘆, I’m pleased to share my results:
• 𝗠𝗼𝗿𝘁𝗮𝗹𝗶𝘁𝘆: 𝟬%
• 𝗔𝘃𝗲𝗿𝗮𝗴𝗲 𝗵𝗼𝘀𝗽𝗶𝘁𝗮𝗹 𝘀𝘁𝗮𝘆: 𝟰.𝟱 𝗱𝗮𝘆𝘀
• 𝗗𝗿𝗶𝘃𝗶𝗻𝗴: ~𝟯–𝟰 𝘄𝗲𝗲𝗸𝘀 𝗽𝗼𝘀𝘁-𝗱𝗶𝘀𝗰𝗵𝗮𝗿𝗴𝗲
• 𝗙𝘂𝗹𝗹 𝗮𝘁𝗵𝗹𝗲𝘁𝗶𝗰 𝗮𝗰𝘁𝗶𝘃𝗶𝘁𝘆: 𝟲–𝟭𝟬 𝘄𝗲𝗲𝗸𝘀 (depending on age, fitness, and preoperative condition)
To complete this discussion, it’s important to recognize that there are indeed 𝘁𝗿𝘂𝗹𝘆 𝗹𝗲𝘀𝘀 𝗶𝗻𝘃𝗮𝘀𝗶𝘃𝗲 𝗵𝗲𝗮𝗿𝘁 𝗽𝗿𝗼𝗰𝗲𝗱𝘂𝗿𝗲𝘀 that are known as “𝗽𝗲𝗿𝗰𝘂𝘁𝗮𝗻𝗲𝗼𝘂𝘀” 𝗼𝗿 “𝗰𝗮𝘁𝗵𝗲𝘁𝗲𝗿-𝗯𝗮𝘀𝗲𝗱” 𝗽𝗿𝗼𝗰𝗲𝗱𝘂𝗿𝗲𝘀 —these do not require stopping the heart or using the heart-lung machine—such as:
• 𝗧𝗿𝗮𝗻𝘀𝗰𝗮𝘁𝗵𝗲𝘁𝗲𝗿 𝗔𝗼𝗿𝘁𝗶𝗰 𝗩𝗮𝗹𝘃𝗲 𝗥𝗲𝗽𝗹𝗮𝗰𝗲𝗺𝗲𝗻𝘁 (𝗧𝗔𝗩𝗥)
• 𝗧𝗿𝗮𝗻𝘀𝗰𝗮𝘁𝗵𝗲𝘁𝗲𝗿 𝗘𝗱𝗴𝗲-𝘁𝗼-𝗘𝗱𝗴𝗲 𝗠𝗶𝘁𝗿𝗮𝗹 𝗥𝗲𝗽𝗮𝗶𝗿 (𝗧𝗘𝗘𝗥 𝗼𝗿 “𝗠𝗶𝘁𝗿𝗮𝗹 𝗖𝗹𝗶𝗽”)
• 𝗣𝗲𝗿𝗰𝘂𝘁𝗮𝗻𝗲𝗼𝘂𝘀 𝗖𝗼𝗿𝗼𝗻𝗮𝗿𝘆 𝗜𝗻𝘁𝗲𝗿𝘃𝗲𝗻𝘁𝗶𝗼𝗻 (𝗣𝗖𝗜) 𝘄𝗶𝘁𝗵 𝗦𝘁𝗲𝗻𝘁𝘀)
These catheter-based procedures represent genuine reductions in physiologic invasiveness.
Ultimately, no operation —conventional, less-invasive/robotic, or catheter-based— should be defined by the size of an incison(s) or by marketing terminology, but by maximal safety, effectiveness, and recovery—achieved through meticulous technique, optimal exposure, and uncompromising outcomes.
The most important thing is for patients to do research, ask questions, and have honest discussions with your doctors regarding your surgeon’s experience and outcomes. Also, it’s important to seek a second opinion whenever feasible. As quickly as technology is expanding, a knowledgeable patient is a safe patient!
——
The views expressed are my own and do not reflect the views of Jefferson Health.
Recent Posts
Why the Heart Team Approach Matters Most
For years, the debate over TAVR versus open heart surgery has shaped cardiovascular medicine. Dr. Raymond Singer shares why the best outcomes come from a collaborative heart team approach focused on the individual patient.
Patient Experience Matters as Much as the Operation
When people think about cardiac surgery, they often focus on the operation itself. But according to Dr. Raymond Singer, the future of heart surgery extends far beyond the operating room. From access to care and patient education to recovery and emotional support, the patient experience is becoming one of the most important measures of healthcare excellence.
I Used to Be an Athlete
After years of long hours, stress, and the demands of a surgical career, Dr. Raymond Singer realized he had drifted far from the healthy athlete he once was. Through consistent lifestyle changes, improved nutrition, exercise, emotional wellness, and the support of modern GLP-1 medications, he lost nearly 60 pounds and discovered that healthy aging begins one decision at a time.
What It Feels Like to Hold a Human Heart
After nearly 9,000 heart operations, Dr. Raymond Singer shares what it feels like to hold a human heart in his hand and explains how studying the remarkable complexity of the heart has strengthened his faith and appreciation for life.
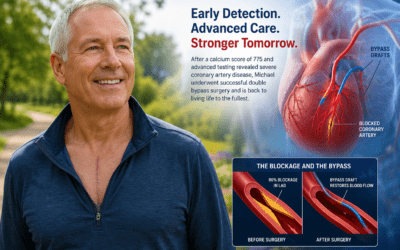
How a Calcium Score Led to Bypass Surgery
When Michael learned his coronary calcium score was 775, he knew something wasn’t right. Although initial stress tests appeared normal, advanced cardiac imaging eventually uncovered severe coronary artery disease with critical blockages. Just 11 days after cardiac catheterization, he underwent successful double bypass surgery and was back home within days, experiencing minimal pain and a remarkable recovery.
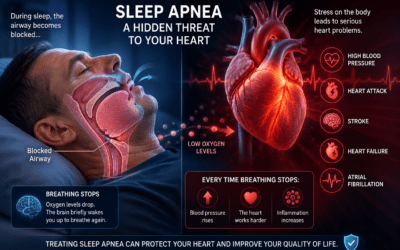
Obstructive Sleep Apnea
Many people think obstructive sleep apnea is simply a nuisance because of loud snoring, but it can have serious consequences for heart health. Repeated interruptions in breathing place tremendous stress on the cardiovascular system and may increase the risk of high blood pressure, atrial fibrillation, heart failure, stroke, and heart attack. Learn the warning signs, risks, and treatment options that can improve both sleep quality and long-term health.
Featured
Pages
- Learn about heart valves. Heart Valves
- Read testimonials. Testimonials
- Did you know I have a consulting firm? Singer Heart/Lung Consulting
- Check out my TedTalk! Defining Success
Links
- Links page with more information about your heart. Links
- Dr. Adam Pick's Site: heart-valve-surgery.com
Questions? Comments?
Reach out to me here:




{kind=link}