Aneurysm vs. Aortic Dissection
Aneurysm
An aneurysm is a dilatation of an artery. Aneurysms can occur in any artery in the body.
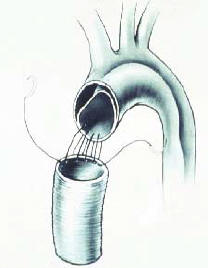
Below is a drawing of an Aneurysm of the Ascending

Aneurysm
The following video describes a complex operation for a patient who has an aneurysm of the proximal ascending aorta, known as the “aortic root.” The procedure is referred to as an “aortic root reconstruction.” In addition to repairing the aneurysm, the aortic valve is replaced and the patient’s left and right coronary arteries are re-implanted into the bio-prosthetic valve-conduit.
I used a Medtronic Freestyle® Porcine (Pig) Root. The advantage of this biologic valve is that the patient will not need Coumadin.
Turn on your speakers because I describe the entire procedure as you watch the video!
Aortic Dissection
A fascinating disease that is often confused with aneurysm is known as aortic dissection.
An aortic dissection is a tear of the inner lining of the artery. The older literature is confusing because it used to refer to this disease as a “dissecting aneurysm.” However, the current and proper terminology is to distinguish aortic aneurysms from aortic dissections.
The differentiation is quite important:
Aortic aneurysms are usually caused by hardening of the arteries (atherosclerosis), whereas aortic dissections are usually caused by a connective tissue disorder and/or high blood pressure. The most infamous connective tissue disorder associated with aortic dissection is Marfan’s disease, but there are others.
Though high blood pressure (hypertension) can be associated with both aortic aneurysms and aortic dissections, high blood pressure is particularly a dangerous cause of aortic dissections.
The danger is also different:
Aortic aneurysms
Aortic aneurysms can enlarge to the point where they rupture, causing sudden blood loss and death. If an aneurysm is found before rupturing, the surgery to repair the aneurysm is usually straightforward and successful. However, once an aneurysm has ruptured, the patient needs emergent surgery and rarely will the patient survive.
Aortic dissections
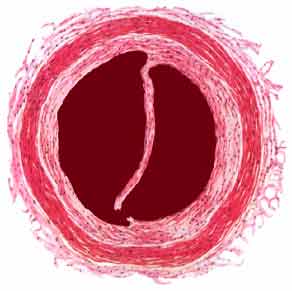
Aortic dissections result in a tearing of the lining of the aorta, causing the blood to “dissect” along the wall of the artery. This causes two channels as shown above. The one channel is known as the “true channel” and the other the “false channel.” With each heartbeat, the artery tears more and more with blood propagating down the false channel blocking off all of the branches of the aorta.
Aortic Dissection
That means, the patient can suddenly lose blood flow to the heart, the brain, the spinal cord, the abdominal organs and the legs. Without immediate surgery, the patient will most certainly die. Though a formidable procedure, many patients will survive repair of an aortic dissection if they can get to the operating room (with an experienced team) quickly.
A while ago, actor John Ritter died from an aortic dissection. The diagnosis was not suspected right away. Unfortunately, the diagnosis of aortic dissection can be missed by inexperienced medical personnel because some of the symptoms can be “away from the heart” such as stroke, back pain, abdominal pain, and lack of blood flow to the legs.
Case Report 1: Aortic Dissection
Below is a CT scan of the chest showing an aortic dissection.
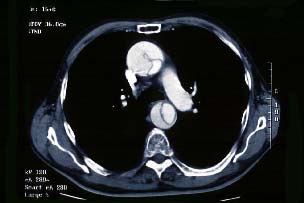
CT of Aortic Dissection
Note the line within the ascending and descending aorta. That’s the torn inner lining!
Below, the ascending aorta is replaced with prosthetic tube and the distal torn artery is repaired.
Artery Repair
The artery is repaired by sewing the layers together usually with a combination of suture, biologic glue, and Dacron cloth and tubes.
Below is a picture of how we use BioGlue® (made by CryoLife Corporation) to help repair the aorta.
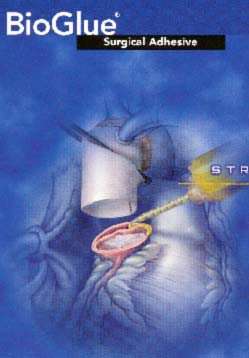
BioGlue®
Case Report 2 – Aortic Dissection
Here is an interesting case of a man who had an aortic dissection repair in the past, but returned with an infection of a prosthetic valve. Below is the MRI of the aortic arch showing a chronic aortic dissection.
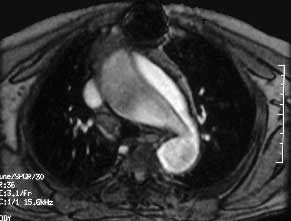
Chronic Aortic Dissection
I had to remove the infected valve and repair the artery. Below is the infected valve after I removed it from the patient and the “vegetation” (infected material) that was growing on the valve is shown next to it.

Infected Valve
The final repair included replacing the entire aortic arch with a Dacron tube as well as replacing the aortic valve and ascending aorta with a cadaver aortic valve and aorta (homograft complete root reconstruction).
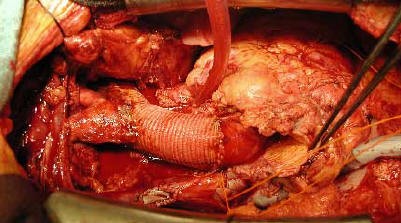
Final Repair
Below is a drawing detailing the above surgery.

Drawing of Dissection Repair
I recently had the opportunity to record and share a complex case involving repair of an ascending aortic aneurysm with complete reconstruction of the ascending aorta and arch. This included re-implantation of the coronary arteries—commonly known as a Bentall procedure—along with replacement of the ascending aorta and aortic arch.
The arch portion required profound hypothermia (18 degrees Celsius) with circulatory arrest, using retrograde cerebral protection to preserve normal brain function.
This operation demonstrates not only the technical precision required for complex aortic surgery but also the importance of careful planning, multidisciplinary teamwork, and innovation in cardiovascular care.
By sharing these videos —always with written permission from the patient— my hope is to provide educational insights into the steps of such high-stakes procedures and to contribute to ongoing discussions within the surgical community about best practices, evolving techniques, and patient outcomes.
Sinus of Valsalva Aneurysm Repair
We recently had the privilege of caring for an 80-year-old gentleman who presented with heart block, bradycardia, and worsening shortness of breath.
Upon further evaluation, he was found to have a ruptured Sinus of Valsalva aneurysm, along with a ventricular septal defect (VSD) and atrial septal defect (ASD). Despite his advanced age, we proceeded with open-heart surgery to repair all three conditions.
These are rare lesions individually, and to encounter them together — particularly in an octogenarian — is truly exceptional.
✅ The Sinus of Valsalva aneurysm was successfully repaired.
✅ Both the VSD and ASD were closed.
✅ Biventricular function was fully restored by the end of the procedure.
✅ He required no significant additional inotropic support postoperatively. As anticipated in such cases, he will likely require a permanent pacemaker.
But most importantly, he is now recovering well — a testament to his resilience, careful perioperative planning, and the dedication of our multidisciplinary team at the 𝐁𝐫𝐮𝐜𝐞 𝐚𝐧𝐝 𝐑𝐨𝐛𝐛𝐢𝐞 𝐓𝐨𝐥𝐥 𝐇𝐞𝐚𝐫𝐭 𝐚𝐧𝐝 𝐕𝐚𝐬𝐜𝐮𝐥𝐚𝐫 𝐈𝐧𝐬𝐭𝐢𝐭𝐮𝐭𝐞, Jefferson Health.
Cases like this remind us that age alone should not be the sole determinant of what is possible. With the right expertise and support, even the most challenging cardiac pathologies can be treated successfully.
With the patient’s kind permission, we are sharing a video of this extraordinary journey.