Congenital Defects
There are many congenital heart defects. The term “congenital” refers to the fact that these defects occur during development of the embryo and as such are present at birth. Unfortunately, these defects are not always recognized immediately at birth.
However, due to the extension use of prenatal ultrasound, many of the most serious congenital defects are suspected even prior to birth.
Congenital heart surgery is a specialty all to its own. Having said that, there are a number of cardiac surgeons who do both adult and congenital heart surgery.
During my three year fellowship in cardiothoracic surgery at Jefferson University Hospital, I spent 6 months at the Children’s Hospital of Philadelphia under the director of one of the world’s most famous congenital heart surgeons, Dr. William Norwood.
Dr. Norwood is best known for his pioneering work for children who are born with a single ventricle (pumping chamber of the heart) instead of the usual two chambers. The Norwood Procedure has has saved the lives of thousands of children worldwide who would have otherwise died.
There are a few congenital heart defects that may be seen for the first time in adulthood.
Two of the most common are atrial septal defects and bicuspid aortic valves.
In addition, because of the proliferation of heart surgery on children over the past two decades, we are now seeing a lot of adults who were operated on when then were young for congenital heart problems. Indeed, it is sometimes difficult to know what to do with these patients since they combine complex congenital anatomy with adult problems. Some have advocated developing a field of “adult congenital heart disease.” For now, many of these adults are actually still followed at pediatric hospitals.
Bicuspid Aortic Valve
The normal aortic valve has three cusps (leaflets). Some children are born with only two cusps as shown in the photo to the right.
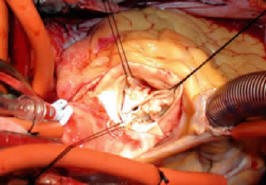
Only Two Cusps
Typically, people can live into their 40’s and 50’s without any problem with from their bicuspid valve. The most common complication from a bicuspid aortic valve in adults is aortic stenosis (the development of calcification on the cusps as shown above that restrict the opening of the valve). Once this occurs to a significant degree, the valve needs to be replaced.
Here you can see videos about Aortic Valve Replacement Videos.
There are more details about Aortic Valve Surgery here.
Quadricuspid Aortic Valve
Quadricuspid Aortic Valve is a rare congenital cardiac defect usually diagnosed incidentally. It is characterized by the presence of four cusps, instead of the usual three found normally in the aortic valve. While patients with this rare finding often develop aortic regurgitation later in life, some patients develop stenosis, while others may remain asymptomatic. Therefore, it is important to regularly follow up these patients for early signs of aortic valve dysfunction.
This adult patient has very rare combination of a quadricuspid aortic valve with both aortic valve stenosis and regurgitation, along with congenital mitral valve stenosis and regurgitation, and will therefore undergo a double heart valve replacement. We will video the procedure and photograph the valves for a case report to share with our cardiology and cardiac surgery colleagues in scientific forums.

Atrial Septal Defects
Below is a drawing of the most common form of atrial defect seen in adults, the so-called “Secundum Atrial Septal Defect.” You will note that there is an opening between the the right and left atrial chambers. That is to say, there is a defect in the atrial septal wall.

There is a lot of interesting discussion concerning human development in the embryo that explains how and why this occurs, but is beyond the scope of my website.
More importantly, patients may go well into adulthood without having this defect picked up. The patient may or may not have a murmur. Shortness of breath and decreased exercise tolerance may be associated with this problem.
Also, patient’s can develop a paradoxical embolism, meaning that a blood clot from the legs can travel to the heart and cross over to the left side and go to the brain causing a stroke (as opposed to the usual pathway of going to the lungs and causing a pulmonary embolism).
Standard, time-tested, surgical correction of an atrial septal defect in an adult involves a relatively simple procedure of sewing a patch over the hole. The patch material used may be a piece of the patient’s own pericardium. Newer patched made of an ultra-thin polyester are very easy to use and work very well.
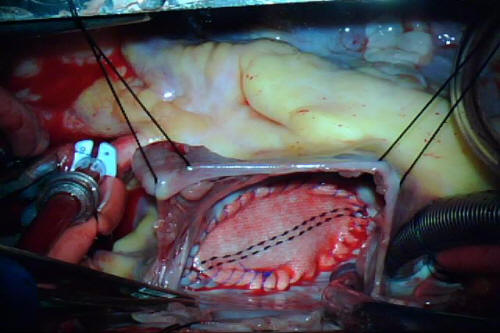
Operative Photograph from a 34-Year Old Woman with a Large Secundum Atrial Septal Defect (ASD) Repair with a Hemashield Polyester Patch
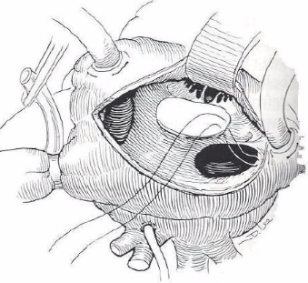
Drawing of an ASD Patch
Below is the video of the operation pictured above. Please turn on your speakers to hear my description of the procedure:
As with many other areas of cardiac surgery, the interventional cardiologists are devising ways of closing these atrial septal defects without surgery. There are devices available today whereby a cardiologist in the cardiac catheterization laboratory will insert a device through a catheter into the heart that closes off the defect. However, this catheter-based procedure is typically used for smaller defects than the one shown above.
Overlap of techniques among medical and surgical disciplines is increasing in healthcare due to the constant development of new technology. That’s why is more important than ever for medical doctors and surgeons to work as a team. And, even more important for patients to be informed, ask questions, and seek a second opinion whenever feasible.

